The average physician spends over 3 hours daily on documentation and EHR work, according to the AMA. That number hasn’t improved in years. Medical transcription services were supposed to fix the documentation problem. Instead, they moved it. Notes came back hours or sometimes days later, were coded incorrectly, and still required physician review. The physician just did the same work in two steps instead of one. This article breaks down the real difference between medical transcription and an AI medical scribe in 2026, where each belongs, and what most physicians evaluating clinical documentation solutions still miss.
What Medical Transcription Services Actually Deliver
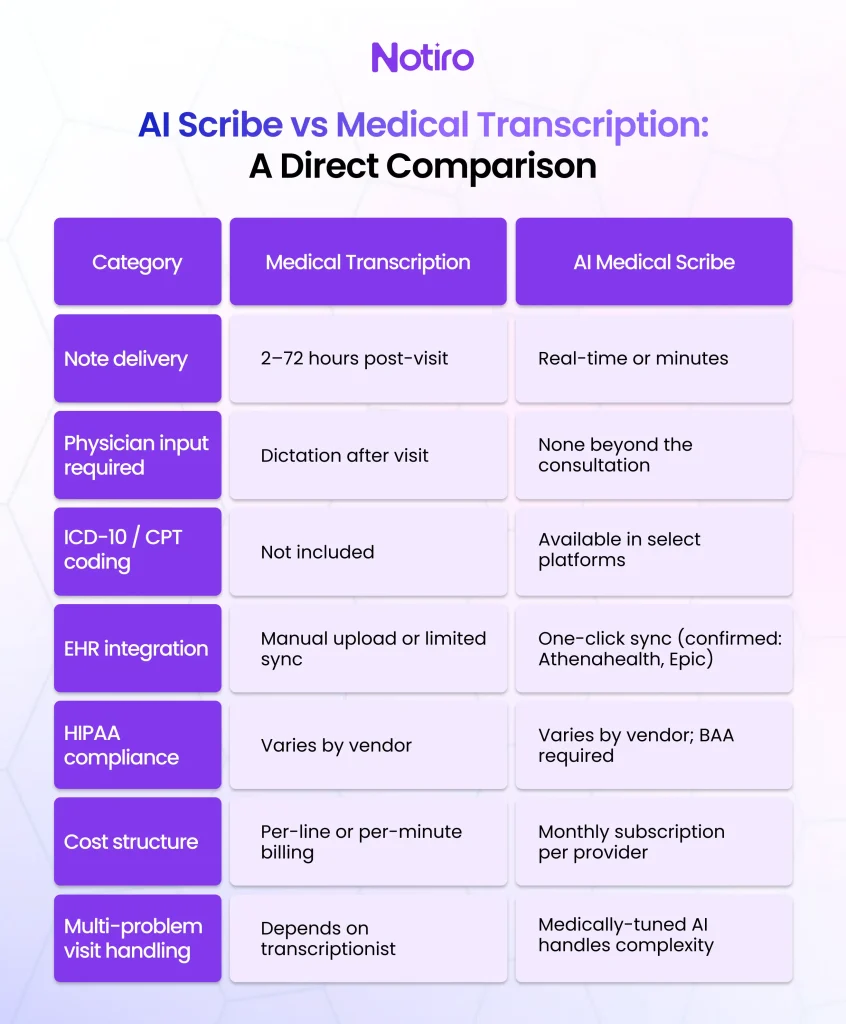
Medical transcription services convert physician dictation into written clinical notes. The physician records their encounter summary after seeing a patient. A transcriptionist, human or software-assisted, types that dictation into a structured document. The finished note is returned to the practice within 2 hours to 3 days.
This workflow has served healthcare for decades. For certain use cases, it still holds value. Highly specialized procedures, legally sensitive documentation, and settings where real-time AI processing is not available may still rely on human transcription for accuracy.
The fundamental problem is timing. A note that returns 24–72 hours after the patient leaves is not a real-time clinical record. The physician cannot reference it for same-day follow-up decisions. Billing cannot begin until the note closes. Staff cannot access documentation that is still in the queue. When a physician sees 20 patients in a day, that lag compounds into a backlog with real downstream consequences for revenue cycle management.
Medical transcription software improved turnaround speed, but it did not solve the underlying workflow gap. The physician still had to dictate after the visit. The note still had to be reviewed and corrected. And the billing codes still had to be manually assigned, because transcription converts speech to text, not speech to structured clinical documentation with billing codes attached.
How AI Medical Scribe Technology Changes the Documentation Model
An AI medical scribe listens to the physician-patient conversation in real time. It does not require the physician to dictate separately after the visit. The AI captures what was said, structures it into a clinical note (SOAP, H&P, or POMR format), and delivers a draft note before the physician reaches the next exam room.
The documentation workflow shifts from a retrospective to a concurrent model. The physician is not creating a note after the fact. The note is being built during the encounter.
Leading AI documentation platforms, such as Notiro, extend this real-time model beyond simple note-taking. By using AI to capture clinical conversations, automatically structure documentation, and prepare downstream workflows, Notiro helps physicians spend less time charting and more time focusing on patient care. The result is fewer manual handoffs, fewer documentation errors, and a significantly faster path from encounter to completed chart.
For practices where time per visit is the primary constraint, this distinction matters. Physicians who dictated notes after seeing patients spent significant time reconstructing conversations from memory. That reconstruction introduced both omissions and inaccuracies. Real-time ambient capture eliminates the reconstruction step entirely.
By 2025, roughly 40% of US physicians had adopted AI documentation tools, according to AMA survey data. The question in 2026 is not whether AI scribes work. It is whether the AI scribe a physician is using actually automates the complete documentation and billing workflow, or just the note.
The cost comparison consistently favors AI scribes when total time is factored in. Medical transcription services typically charge per line or per audio minute, creating variable costs that scale with patient volume. A solo physician seeing 100 patients per week incurs significant monthly transcription costs before accounting for the time required for review and correction.
The biggest efficiency gains come from platforms that automate multiple administrative tasks simultaneously. Notiro uses AI not only to generate clinical notes, but also to organize encounter data, support coding workflows, and streamline chart completion. When physicians evaluate documentation solutions, the true comparison is not transcription costs versus software costs; it is the amount of clinician time each platform returns to the practice.
The Problem Most Physicians Don’t Catch: AI Scribes That Stop at the Note
Most automated medical documentation tools write the note. That is where the feature set ends. The physician burnout problem is not solved by a faster note alone. Documentation burden in 2026 includes three distinct workflows: gathering patient history before the visit, capturing the encounter during the visit, and closing the chart with accurate billing codes after the visit.
Most AI scribes for healthcare cover only the second stage. They record the encounter and return a note. The physician still has to manually assign ICD-10 and CPT codes from memory after seeing 20 patients. According to CMS, ICD-10 has over 70,000 codes, and CPT has over 10,000. Manual post-visit code selection under time pressure is a systematic source of undercoding: the physician documents a lower-complexity visit than was actually delivered and bills accordingly.
Undercoding costs thousands of dollars per month in missed reimbursement. This is not a billing department problem. It is a documentation workflow problem that begins the moment a physician rushes through the code selection screen at the end of a long day.
Notiro addresses all three stages and is one of the few AI-powered documentation platforms designed to automate the entire clinical documentation workflow rather than a single task. Before the visit, Patient Intake AI collects the patient’s presenting complaints and history directly. During the visit, the ambient scribe captures and structures the consultation in real time. After the visit, Notiro auto-suggests ICD-10 and CPT codes drawn from the visit audio and note, then syncs to the EHR with one click. By reducing manual data entry and helping physicians make more accurate coding decisions, Notiro helps practices save time, reduce documentation errors, and improve reimbursement outcomes. No other Tier 1 competitor, including Freed AI, Heidi Health, or Nabla, offers automated ICD-10 and CPT coding at this level. DeepScribe offers comparable billing automation at $350–$500 per provider per month, a price point inaccessible to most solo practices and small groups.
Before the visit, Patient Intake AI collects the patient’s presenting complaints and history directly. During the visit, the ambient scribe captures and structures the consultation. After the visit, Notiro auto-suggests ICD-10 and CPT codes drawn from the visit audio and note, then syncs to the EHR with one click. No other Tier 1 competitor, including Freed AI, Heidi Health, or Nabla, offers automated ICD-10 and CPT coding at this level. DeepScribe offers comparable billing automation at $350–$500 per provider per month, a price point inaccessible to most solo practices and small groups.
HIPAA, Compliance, and What Every Physician Must Verify
Every healthcare documentation tool, whether medical transcription software or an AI scribe, must sign a Business Associate Agreement (BAA) with the physician’s practice. Under HIPAA, any vendor processing Protected Health Information must have a BAA in place. A physician using an AI scribe without a confirmed BAA from that vendor is potentially in violation of HIPAA, regardless of how well the tool performs clinically.
HIPAA-compliant AI scribes carry a BAA and process patient audio through a secure, compliant infrastructure. The question physicians should ask any vendor, AI scribe, or transcription service is direct: Do you sign a BAA? Do you use patient audio to train your AI models? Where is patient data stored and for how long?
Notiro is HIPAA compliant and provides a BAA to every practice. Patient data security is a non-negotiable baseline for any clinical documentation solution, not a premium feature.
Which Healthcare Documentation Tool Fits Which Practice in 2026
Medical transcription services still have a place in healthcare. High-stakes procedural documentation, legal record creation, and settings where real-time ambient AI is not appropriate, such as operating rooms with complex multi-voice environments, may still benefit from human review. The precision of an experienced medical transcriptionist in a surgical specialty context is not yet fully replaced by AI alone.
In outpatient primary care, family medicine, internal medicine, and psychiatric practice, the math has decisively shifted toward AI scribes for healthcare. Solutions such as Notiro demonstrate why this shift is accelerating. Rather than functioning as a standalone note-taking tool, Notiro uses AI to connect patient intake, documentation, coding support, and EHR workflows into a single process. This integrated approach reduces administrative friction across the care journey and helps clinicians complete documentation with greater consistency and fewer manual steps.
Real-time note generation, direct EHR integration with platforms such as Athenahealth and Epic, and automated billing code suggestions remove the three main bottlenecks that medical transcription services have never resolved: turnaround delays, manual code selection, and the physician’s time spent reviewing and correcting documentation after hours.
The physician who is still dictating at 9 PM, reviewing transcriptions before bed, and manually selecting billing codes the next morning is not running an inefficient practice. That physician is using tools designed for a different era of clinical documentation.
The Documentation Problem Medical Transcription Was Never Built to Solve
Traditional transcription converts what the physician says. Modern platforms such as Notiro are built around a different objective: transforming conversations into actionable clinical documentation that supports both care delivery and operational efficiency. By leveraging AI throughout the documentation lifecycle, Notiro helps healthcare teams reduce administrative burden, improve workflow accuracy, and close charts faster without sacrificing clinical quality.
An AI medical scribe captures what actually happened in the room and structures it into documentation that is immediately usable, accurately coded, and ready to sync to the chart. The physician’s cognitive load does not shift after hours. The billing codes are not left to memory.
Choosing between medical transcription vs AI scribe in 2026 is not a question of technology preference. The question is whether the documentation workflow ends at the note or closes the entire clinical loop, from patient intake through chart closure.
Documentation is still the last hour of the physician’s day when it should not be. Notiro automates notes, intake, and billing codes, so the chart closes before the next patient walks in. Start your free trial at notiro, no IT setup, no enterprise contract.