A family physician finishes their last patient at 5:30 PM. The encounter involved hypertension, a new knee complaint, a diabetes medication adjustment, and a question about a colonoscopy referral. Four separate problems. One 15-minute visit. The note is not going to write itself, and neither is the billing code that accounts for the complexity of what just happened.
This is family medicine. Not one problem per visit. Not a tidy SOAP note waiting to be filled in. It is the specialty with the highest patient volume, the widest clinical breadth, and the most documentation per day. The AMA has measured 86 minutes of nightly EHR work specifically for family physicians after clinic hours, paperwork that follows the physician home because the visit day left no time to finish it.
An AI medical scribe can help with that. Most AI scribes only help with part of it. That distinction matters when a family physician is choosing a documentation tool.
What Makes Family Medicine Documentation Different
Family physicians see patients across every age group, every organ system, and every level of urgency, sometimes in the same morning. A 9:00 AM wellness visit can be followed by an acute chest pain complaint, a chronic COPD management check, and a pediatric ear infection by 10:30. Each encounter generates documentation requirements that span preventive care, chronic disease management, and acute care, often in one note.
The family medicine documentation challenge is not just volume. It is a multi-problem visit. A published study in Annals of Family Medicine found that family medicine encounters average 3.05 diagnoses per visit, rising to 3.88 for patients over 65. That is not an unusually complex visit. That is a typical Tuesday morning.
AI scribes were built for exactly this situation. But the version of “AI scribe” that most tools deliver, an ambient recorder that produces a SOAP note, still leaves the family physician finishing the job. The note is written. The billing codes are not. The patient intake was still manual. The EHR sync requires copy-paste.
The Note-Only Problem
Ambient scribing has become standard. Freed AI, Heidi Health, Nabla, and dozens of other tools will listen to a visit and produce a structured clinical note. This matters, and it saves real time. But clinical documentation AI that stops at the note is solving roughly half the workflow problem in primary care.
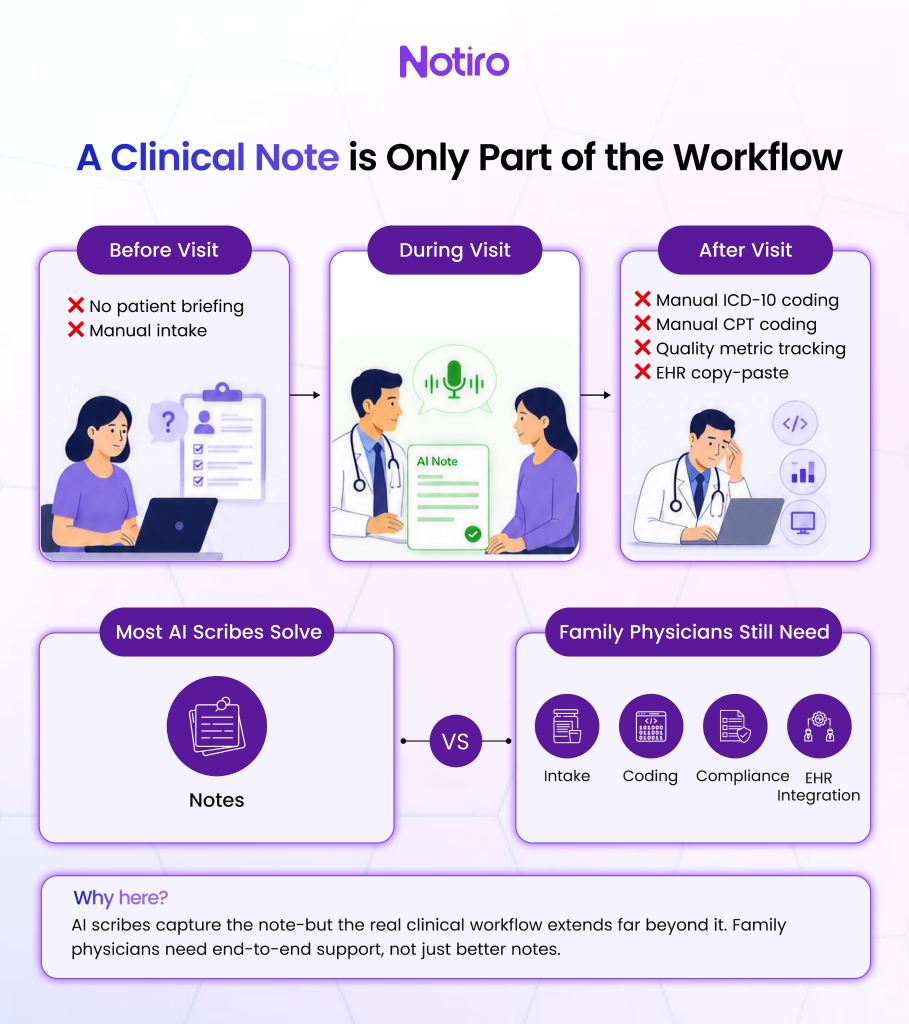
Here are the gaps that show up on a real family practice day.
Before the visit, the physician walks in with no prior briefing. The patient’s presenting complaints, recent medication changes, and relevant history must be collected at the start of the encounter, further eating into the visit time that documentation already compresses.
During the visit, the ambient scribe captures the conversation and produces a note. For a single-problem acute visit, this works well. For a multi-problem chronic care visit, the accuracy of the note depends heavily on how well the tool handles complex, overlapping clinical language.
After the visit: The note exists, but the ICD-10 diagnosis codes and CPT procedure codes do not. They get selected manually, under time pressure, by a physician who is already running behind. Undercoding, selecting a lower-complexity code than the visit warranted, is one of the most persistent billing errors in outpatient primary care. It happens not by intent but because of the structural impossibility of thorough manual coding at this pace.
There is a fourth gap that receives less attention: documentation of quality metrics. Family medicine practices participate in MIPS (Merit-based Incentive Payment System) and HEDIS reporting programs that tie reimbursement adjustments to whether specific clinical actions are captured in chartable fields. A scribe who misses a flagged colonoscopy or an undocumented depression screening leaves compliance revenue on the table alongside the billing gap.
What the Evidence Shows
A study across Mass General Brigham and Emory Healthcare, published in JAMA Network Open in 2025, found a 21.2% absolute reduction in burnout prevalence at Mass General Brigham after 84 days of AI scribe use, dropping from 52.6% to 30.7%. The effect was most pronounced among primary care physicians, the specialty group carrying the highest multi-problem documentation load.
The data make the case for AI scribes in family medicine. What it cannot determine is whether the chosen tool covers the full workflow or only the note.
Why ICD-10 and CPT Coding Matter More Here Than Anywhere Else
Family medicine has the broadest ICD-10 coding footprint of any outpatient specialty. A single clinic day can require codes spanning diabetes (E11.x), hypertension (I10), musculoskeletal complaints (M79.x), preventive care (Z00.x), and behavioral health (F41.1), across visit types that each carry different CPT complexity levels.
The CMS ICD-10 system contains more than 70,000 codes, and the CPT contains more than 10,000. Manual post-visit code selection done at the end of a 20-patient day under time pressure is a structurally unreliable process. The family physician who selects 99213 when the visit warrants 99214 is not making a coding error. They are making a time-pressure decision that costs the practice money every time it happens.
Notiro’s ICD-10 and CPT coding automation surfaces diagnosis and procedure codes from the visit audio and clinical note before the chart closes. Among the major AI scribe competitors, Freed AI, Heidi Health, and Nabla do not offer this at all. DeepScribe does, at $350 to $500 per provider per month. Notiro delivers the same automation to solo practices and small groups.
The Full Clinical Day in Family Medicine
The Notiro platform covers three stages that map directly to how a family physician moves through a patient day.
- Before the visit, Patient Intake AI collects presenting complaints, symptoms, medication history, and relevant background information from the patient. The physician walks in already briefed. None of the Tier 1 AI scribe competitors offer this.
- During the visit, the ambient AI scribe listens to the physician-patient conversation and generates notes in SOAP, H&P, or POMR format with multi-problem visit support built in. It runs on mobile with no additional hardware required.
- After the visit, ICD-10 and CPT codes are automatically suggested. The note and codes sync to the EHR in one click via confirmed EHR integration with Athenahealth and Epic. The chart closes before the next patient walks in.
Heidi Health uses the phrase “full clinical day” as a positioning statement. Notiro’s three-stage workflow makes it a product description.
What to Ask Before Choosing an AI Scribe for Family Practice
Any AI scribe marketed for family medicine should clear four criteria before a practice commits: how it handles multi-problem visits (trial it on a chronic disease encounter, not a wellness check), whether it auto-suggests ICD-10 and CPT codes, whether it executes a signed BAA before any patient audio is captured, and whether it integrates directly with the EHR rather than requiring copy-paste. For family practices using Athenahealth or Epic, that last point matters more than any feature demo.
The Real Question Before Choosing an AI Scribe for Family Medicine
The documentation burden in family medicine is not a paperwork inconvenience. It is the mechanism through which primary care physicians lose evenings, undercode visits, and eventually leave the specialty they trained for. A 21.2% drop in burnout in 84 days is not a marginal improvement. It is the difference between a sustainable career and one that ends too early.
An AI scribe that writes the note addresses part of this. A platform that covers patient intake before the visit, multi-problem documentation during it, and ICD-10/CPT auto-coding after it addresses the full workflow. That is the question worth asking before choosing: is this tool solving the note problem or the clinical-day problem?
Start Documenting Smarter, Not Longer
Family medicine visits average 3.05 diagnoses each, and a note-only scribe closes none of the gaps that follow: no billing codes, no intake prep, no quality metric flags, no EHR sync. Notiro covers all three stages of the family physician’s clinical day: patient intake before the visit, ambient scribing during the visit, and ICD-10/CPT coding after the visit, in one platform built for practices of any size. Start your free trial at Notiro, no IT setup, no enterprise contract.