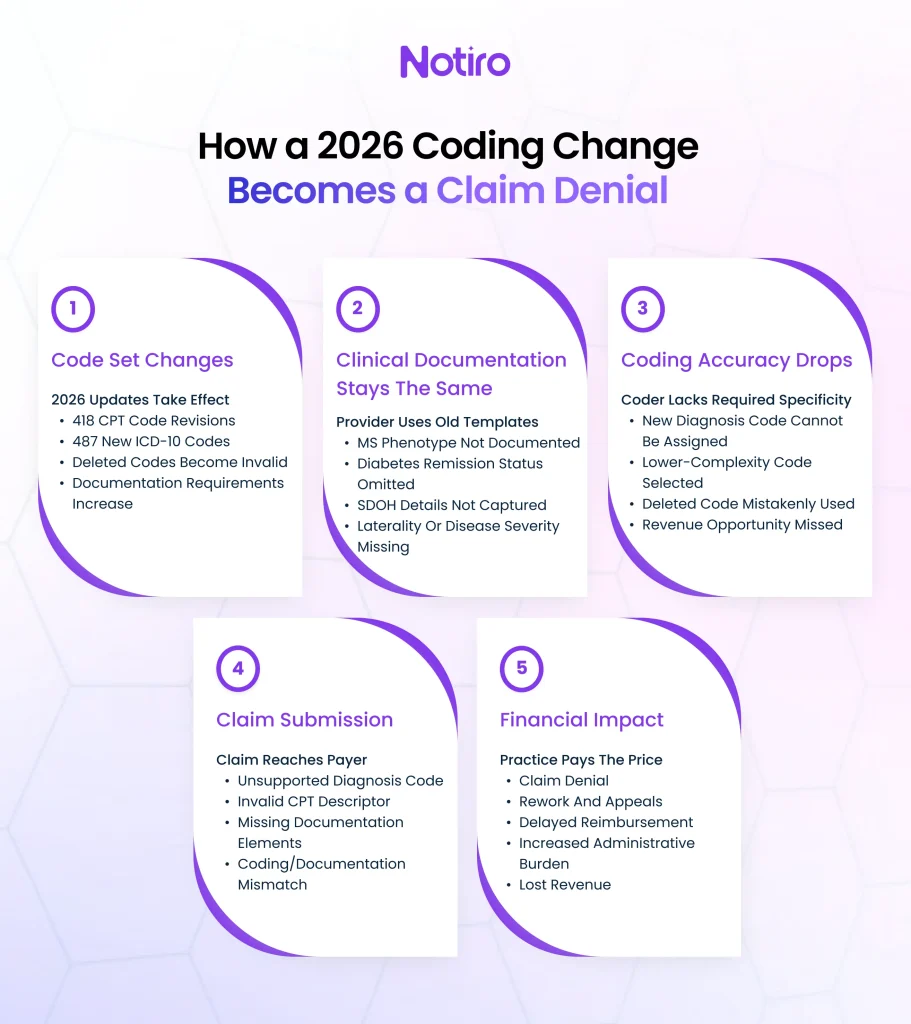
Most practices discover coding changes when a denial arrives. By then, the documentation is filed, the visit is billed, and correcting it costs more time than anyone planned for. The 2026 CPT code changes and ICD-10 2026 update are not routine adjustments. They represent one of the largest coding overhauls in recent years, with deletions that trigger automatic rejections and specificity requirements that cannot be met without updated documentation. This article breaks down exactly what changed, which specialties carry the highest risk, and what a practice needs to address before the next billing cycle.
Why the 2026 CPT Code Changes Are Different From Prior Years
The scale of this year’s list of 2026 CPT code changes is not typical. The AMA introduced 418 total editorial changes, with 288 new codes spanning evaluation and management, remote monitoring, behavioral health, and AI-assisted diagnostics. These changes reach into everyday outpatient workflows, not just specialty surgical codes.
CMS 2026 CPT code changes align Medicare reimbursement directly with the AMA’s updated set. Any code in a practice’s charge master that maps to a deleted or revised descriptor now carries immediate claim risk. A revised descriptor does not bill identically to its predecessor; payers apply the new definition rather than the prior workflow.
For many practices, keeping pace with annual coding changes has become increasingly difficult because the burden falls on physicians and billing staff to remember hundreds of revisions. Leading AI-powered documentation and coding platforms such as Notiro help reduce that risk by automatically surfacing current ICD-10 and CPT code suggestions directly from patient encounters. By connecting documentation and coding workflows, practices can spend less time managing code updates manually and more time focusing on patient care.
The deletion pattern this cycle is consequential. Legacy codes across vascular surgery, audiology, and radiology were removed and replaced with territory-based and complexity-based replacements. A practice filing a deleted code after January 1, 2026, receives a full rejection, not a reduced payment.
What the ICD-10 2026 Update Changed, By Specialty
The FY 2026 ICD-10 2026 update took effect October 1, 2025, carrying 487 new diagnosis codes, 38 revisions, and 28 deletions (source: CDC). Every chapter except two was affected. The highest-impact areas by specialty are below.
Neurology carries the sharpest immediate exposure. The general multiple sclerosis code G35 was deleted and replaced with a subcategory series requiring documentation of the specific MS phenotype (relapsing-remitting, primary progressive, or secondary progressive) and whether the disease is currently active. The old code no longer exists. Any claim using G35 after October 1, 2025, produces an automatic denial.
Primary care and internal medicine face expanded specificity requirements for diabetes. A new code, E11.A, captures type 2 diabetes in remission, requiring explicit provider documentation of remission status. Without that language in the note, the code cannot be applied, and the associated reimbursement is lost.
This is where AI-assisted documentation is becoming increasingly valuable. Notiro uses AI to capture clinical conversations and generate structured notes that reflect the specificity modern coding requires. When documentation accurately records details such as remission status, disease progression, or encounter complexity, coding teams are better positioned to apply the correct diagnosis codes and avoid preventable denials.
Behavioral health gains new CPT recognition for audio-video and audio-only telehealth services, now listed in CPT appendices P and T. The CMS 2026 CPT code changes validate these as equivalent to in-person encounters, which is directly relevant for rural practices where in-person access is structurally limited.
Social determinants of health now have granular codes covering financial insecurity, utility instability, housing instability, and war exposure. These affect risk adjustment and population health reporting, and payers are beginning to require them for specific patient cohorts.
The List of 2026 CPT Code Changes With Direct Outpatient Billing Impact
Remote physiologic monitoring was restructured in the CMS 2026 CPT code changes. Two new codes, 99445 and 99470, cover device supply and initial treatment management. Existing codes 99453, 99454, 99457, and add-on 99458 were revised. Providers can now bill for monitoring periods as short as 2–15 days within a 30-day cycle, down from the prior 20-day threshold. Practices running RPM programs that have not updated billing workflows will underbill or file incorrect codes.
Workflow changes like these often create operational gaps because staff must simultaneously adapt documentation, coding, and billing processes. AI-powered platforms such as Notiro help healthcare teams stay aligned by generating encounter documentation and coding recommendations from the same source of truth, reducing administrative complexity and minimizing opportunities for human error.
AI-assisted diagnostics entered Category I CPT status for the first time. New codes cover augmentative software analysis for coronary plaque assessment, perivascular fat analysis for cardiac risk, and multispectral imaging for burn wounds. These were Category III experimental codes. They are now standard billable services. Practices that offer these services and bill them incorrectly are leaving reimbursement unclaimed.
Immunization counseling now has standalone billable codes. Providers can bill for vaccine counseling without a corresponding vaccine administration. For high-volume preventive care practices, this is a direct revenue capture opportunity that did not exist before.
What Practices Consistently Get Wrong During Code Update Cycles
The failure point is not awareness of the changes. Most practices receive the updated list. The failure is the gap between knowing a code change and updating the documentation that actually supports it.
A deleted or revised ICD-10 code means the diagnosis note must now meet a higher specificity threshold. The note needs to state the MS phenotype, the diabetes remission status, and the injury’s laterality. If that language is absent, no coder can apply the new code correctly, regardless of whether the billing software is updated.
Undercoding in this context is the systematic result of documentation that no longer matches the current code set. A physician charting a complex chronic visit using pre-2026 template language generates a note that supports only a lower-complexity code, even when the encounter warranted full-specificity reimbursement. The AMA’s ICD-10 library contains over 70,000 codes; manual post-visit selection under time pressure is where that specificity consistently gets lost (source: CMS).
How AI Coding Handles Annual Code Updates Without Burdening the Physician
An AI medical scribe that only produces the note does not solve the coding problem. The note is one input; code selection is a separate step, and it is where revenue leaks occur under a new code set.
As one of the leading AI-powered medical documentation and coding solutions, Notiro captures the visit from consultation audio and generates both the clinical note and ICD-10 and CPT code suggestions before the chart closes. Its AI analyzes the clinical conversation in real time, helping providers document more efficiently while reducing the coding errors that commonly occur during manual post-visit workflows. When a new code cycle takes effect, the suggestions reflect the current set, not a physician’s memory of last year’s codes. The practice manager does not need to retrain clinical staff on 288 new CPT descriptors; the auto-coding surfaces what the visit actually supports.
The physician reviews, adjusts if needed, and syncs to the EHR in one click. UCSF research found that AI scribe adopters earn approximately $3,000 more per year and see approximately one more patient per week (source: UCSF, cited in Notiro materials). The coding accuracy layer compounds that, because it applies full-complexity codes the visit supports, not the lower-complexity codes selected at the end of a 20-patient day.
This review-first approach keeps clinicians in control while allowing AI to handle much of the administrative workload. Instead of searching through annual coding updates or manually matching diagnoses to evolving code sets, providers receive decision support at the point of documentation, improving efficiency without disrupting existing workflows.
Preparing for the Next Code Cycle Before It Becomes a Denial Problem
The ICD-10 2026 update is already active. The list of 2026 CPT code changes took effect January 1. Practices that have not audited their highest-volume codes against the current set are billing on definitions that no longer exist.
Three steps produce the most direct impact. Map the practice’s top diagnosis and procedure codes against 2026 deletions and revisions, specifically the ones affecting the practice’s specialty mix. Update documentation templates to capture the specificity the new codes require: phenotype for MS, remission status for diabetes, and SDOH detail for qualifying populations. Then monitor payer response on revised codes through the first billing cycle and track denial spikes in the categories that changed.
Many organizations are also incorporating AI-enabled documentation and coding tools into this process. Platforms like Notiro can help practices identify code-supported documentation before claims are submitted, reducing the likelihood that coding changes surface later as denials, rework, or lost reimbursement.
The physician burnout literature consistently identifies documentation burden as the primary driver of after-hours charting (source: AMA). Layering a code update cycle onto an already heavy documentation load without structural support does not produce better compliance. It produces coding fatigue and the revenue loss that follows.
Annual code cycles are healthcare’s most predictable revenue risk, and still among the least systematically managed. The 2026 updates carry deletions that produce automatic denials and specificity thresholds that require documentation changes at the point of care, not in the billing queue after the fact.
Practices with strong documentation workflows absorb code-cycle changes without disrupting revenue. Those relying on manual post-visit coding, outdated templates, and under-updated charge masters absorb those changes as denial spikes, lost reimbursement, and staff hours spent on appeals. The structural fix is not more training; it is building the code update into the documentation workflow before the note closes.
Coding changes should not land in a denial queue before a practice notices them. Notiro auto-suggests ICD-10 and CPT codes from each visit’s audio and note before the chart closes, so the current code set is applied at every encounter, not caught in a billing audit weeks later. Start your free trial at notiro. No IT setup, no enterprise contract.