An oncologist can explain a treatment plan in fifteen minutes and still spend another thirty documenting it afterward.
Not because the care was unclear, but because modern healthcare requires every decision, risk, medication change, and follow-up step to be translated into billable, defensible documentation.
That process sounds administrative. However, in real clinical workflows, it directly affects reimbursement, compliance, audit readiness, and operational efficiency.
Evaluation and management coding depend heavily on documentation quality. If the note lacks clinical reasoning, supporting details, or clarity, the selected code becomes difficult to defend. On the other hand, overly bloated notes filled with copied text can make the real medical decision-making harder to identify.
Therefore, CPT code automation is not simply about coding faster. It is about helping clinical documentation accurately reflect the complexity of care delivered.
What Are E/M Codes?
Evaluation and management coding is used for many common healthcare encounters, including office visits, follow-ups, consultations, and hospital care.
The American Medical Association(AMA) updated E/M guidelines to allow clinicians to select many office visit codes based on either total time or medical decision making(MDM). The goal was to reduce unnecessary documentation burden while improving clarity around patient care complexity.
In simple terms, E/M coding asks one important question: Does the documentation support the level of service being billed? That is where many clinics experience difficulty.
Why E/M Coding Accuracy Is Difficult
E/M coding requires more than documenting symptoms and treatment plans. The note must clearly show:
- Problems addressed during the visit
- Clinical reasoning
- Data reviewed
- Risk level
- Medication management
- Follow-up planning
- Time spent, where applicable
For example, a clinician may review imaging, discuss medication risks, adjust treatment plans, and evaluate worsening symptoms during a complex visit. However, if those details are not documented clearly, the selected E/M level may not appear justified.
At the same time, over-documentation creates its own problems. Notes overloaded with copied text or repetitive templates can bury the actual clinical reasoning.
Thus, the issue is not always missing documentation. Sometimes, the issue is documentation that lacks signal and structure. This is why clinical documentation improvement is closely tied to coding accuracy.
The Financial Risk of Incorrect E/M Coding
Incorrect E & M codes can create significant compliance and reimbursement risks. The HHS Office of Inspector General reported that Medicare improperly paid $6.7 billion for E/M services in 2010 due to incorrect coding and insufficient documentation. The report also found that 42% of claims were incorrectly coded and 19% lacked proper documentation.
Although healthcare documentation standards have evolved since then, the underlying challenge remains the same: the billed service must match what the chart can support.
Therefore, coding accuracy is not only a billing concern. It is also a compliance and audit-readiness concern. A code is only as defensible as the documentation behind it.
Why Manual Coding Workflows Create Friction
In many clinics, coding workflows still depend heavily on manual documentation and retrospective review.
Typically, the clinician finishes the visit, completes the note, selects the E/M code, and sends the documentation to billing. Later, coders may return questions if parts of the chart are unclear or incomplete.
This creates additional work for everyone involved. Clinicians already face documentation fatigue. Billing teams then spend time interpreting what happened during the visit instead of reviewing a clearly structured note.
But wait, the issue is not that clinicians do not understand patient care. The issue is that clinical thinking and coding logic are not always documented in the same language.
Clinicians think about diagnosis, risk, treatment decisions, and patient outcomes. Coding systems require those decisions to appear clearly inside structured documentation. That is where CPT code automation becomes useful.
How CPT Code Automation Works
CPT code automation uses AI-supported workflows to help identify coding-ready documentation based on the patient encounter.
In many AI scribe systems, the workflow begins during the visit itself. The system captures the conversation, drafts the note, and organizes clinical details into structured sections. Afterward, the clinician reviews and approves the documentation before final submission.
Automation can help surface:
- Problems addressed
- Tests reviewed
- Medication changes
- Risk discussions
- Follow-up planning
- Time-based documentation
- Missing documentation elements
However, the most important point is this:
Automation should support coding decisions, not replace clinical judgment. The final code still requires clinician and billing review.
How AI Scribes Improve E/M Coding Accuracy
An AI scribe can improve evaluation and management coding accuracy by improving documentation quality before the coding process begins.
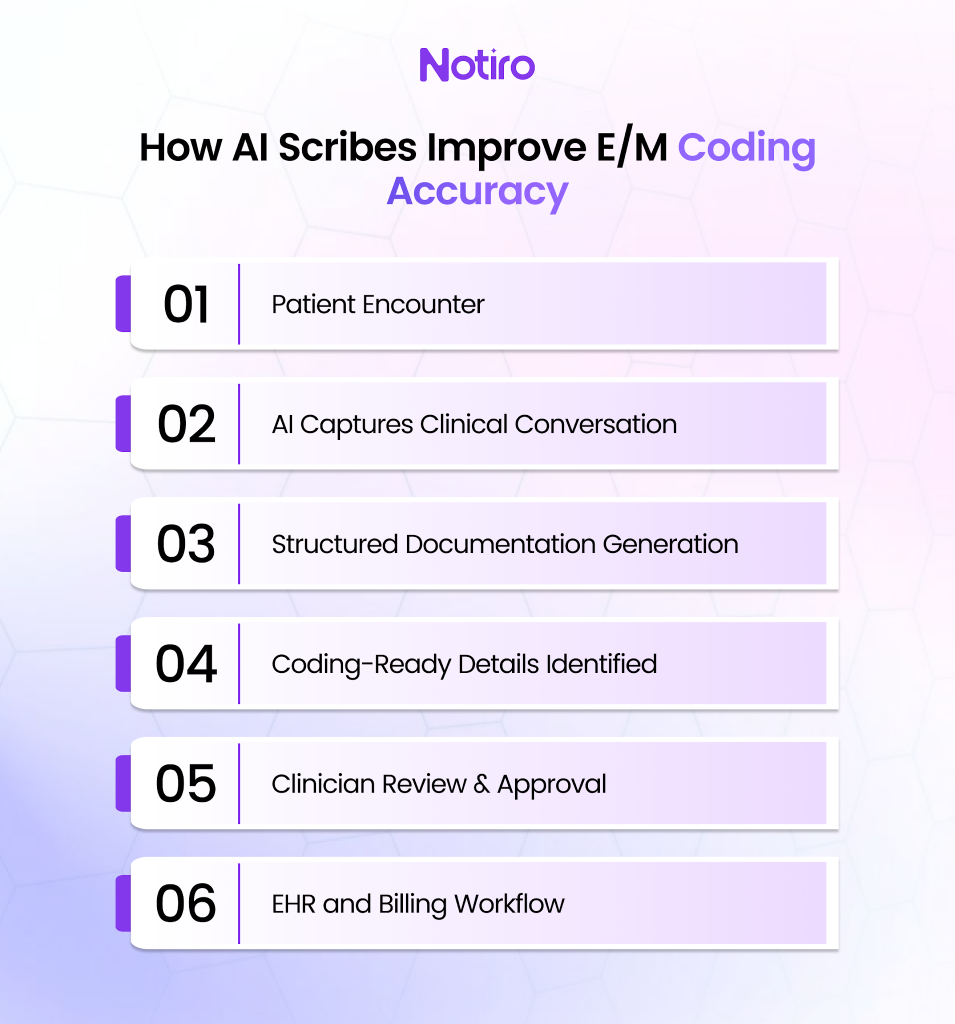
First, it captures encounter details in real time. This reduces the need for clinicians to reconstruct visits later from memory.
Second, it helps structure the documentation more clearly. Medical decision-making elements become easier to identify because the note follows a cleaner format.
Third, AI documentation can reduce missing details. Medication discussions, data review, risk considerations, and follow-up instructions are more likely to remain visible inside the draft note.
Finally, it improves consistency across workflows. Cleaner documentation reduces back-and-forth communication between clinicians and billing teams.
The Centers for Medicare & Medicaid Services notes that when time is used for E/M billing, the medical record should document the total time or appropriately record start-and-stop times.
These are small details that can easily be missed in busy clinics. AI-supported documentation workflows help surface those elements before the note is finalized.
Why Documentation Quality Still Matters Most
CPT code automation cannot compensate for weak clinical documentation. If the note does not clearly explain the medical decision-making process, automation alone should not “upgrade” the code. That would create compliance risk instead of reducing it.
Therefore, the strongest AI workflows focus on documentation support first. A good AI-assisted note should explain:
- What problem was addressed
- Why certain decisions were made
- What risks were discussed
- What data was reviewed
- What treatment plan was selected
- What follow-up is required
In other words, AI should help clinicians tell the clinical story more clearly.
Clinical Documentation Improvement and Coding
Clinical documentation improvement(CDI) connects patient care with billing accuracy and compliance.
For E/M coding, strong CDI workflows help ensure the note supports the service level without unnecessary clutter. A well-structured note should answer:
- What condition was evaluated?
- How complex was the decision?
- What data was reviewed?
- What treatment risks were managed?
- Does the documentation support the selected code?
When those answers are clear, coding becomes more accurate and easier to defend. Thus, CPT code automation should be viewed as part of a broader documentation improvement strategy rather than simply a billing shortcut.
The Future of E/M Coding Is Review-First Automation
The future of evaluation and management coding is not fully autonomous billing.
The better approach is review-first automation. AI captures the encounter, drafts the note, and organizes coding-related documentation elements. After that, clinicians and billing teams verify the final documentation and coding decisions.
This reduces manual burden while preserving accountability and clinical oversight. Most importantly, it helps clinicians spend less time rebuilding the visit after the patient has already left.
Notiro Helps Clinics Create Coding-Ready Documentation
Clinics need documentation workflows that support coding accuracy without adding more administrative complexity.
Notiro helps capture patient conversations in real time, generate structured clinical notes, and support coding-ready documentation that clinicians can review and approve before EHR sync.
With SOAP and HPI templates, contextual awareness, smart phrases, AI medical coding support, HIPAA-compliant security, and EHR integration workflows, Notiro helps reduce documentation friction while keeping clinicians in control of the final note.
So, the outcome becomes simple and clear with cleaner documentation, stronger coding support, and less time spent correcting charts after the visit ends.