A physician dictates a patient visit. The note goes into the chart. Somewhere between that dictation and the final record, a decimal shifts, a drug name is misread, or a critical allergy disappears. The patient returns for their next appointment, and the error travels with them. Medical transcription errors are not rare exceptions. They are a persistent, well-documented failure point in healthcare documentation that affects patient safety, legal liability, and practice revenue. This article makes the cost of inaccuracy visible and shows where AI-driven documentation is actually closing that gap.
How Medical Transcription Errors Enter the Clinical Record
The pathways for transcription errors in healthcare are predictable. A physician works through a 20-patient day, dictates notes under time pressure, and relies on downstream processes to capture those words accurately. That reliance creates exposure at every handoff.
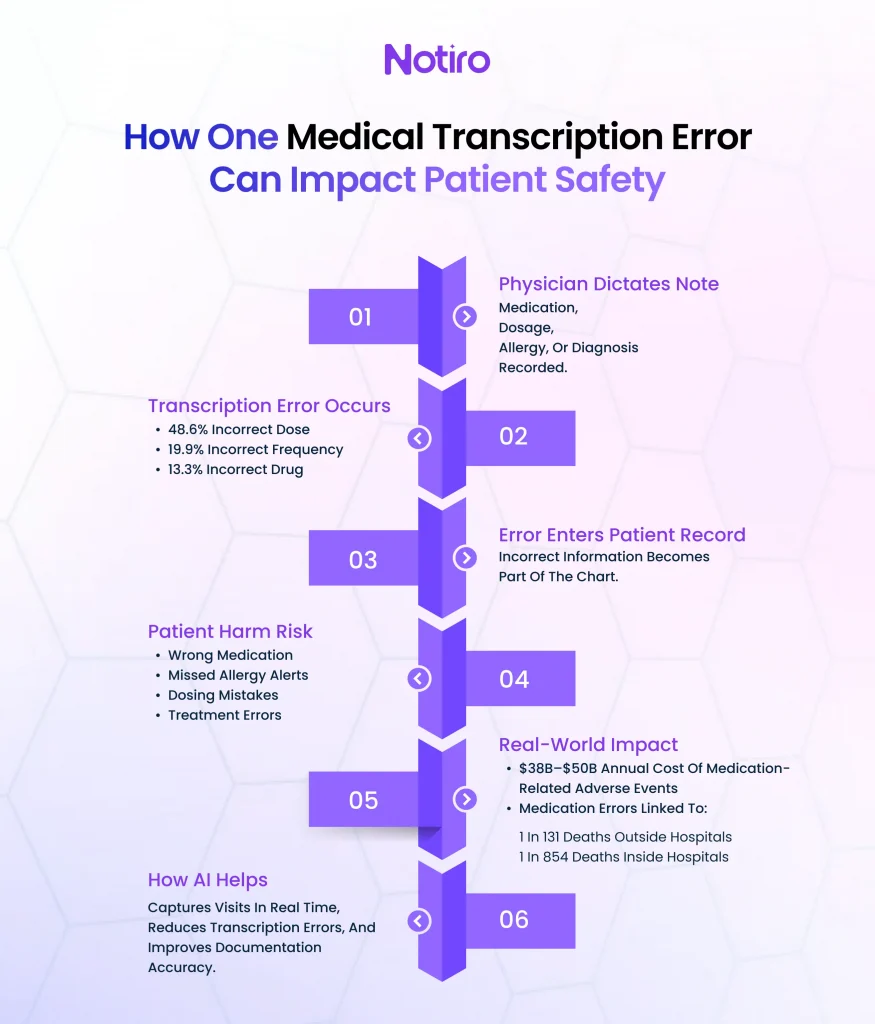
The most common transcribing errors identified in research are incorrect dose (48.6%), incorrect frequency (19.9%), and incorrect drug (13.3%), according to a national medication error reporting analysis. These surface across hospital and outpatient settings alike, most often at the stage where a prescription is transcribed from dictation into an order system.
Manual data entry under cognitive load is structurally unreliable. When a physician dictates “ten milligrams” and the note captures “one hundred milligrams,” that is not carelessness. It is the predictable result of a system that pits transcription accuracy against time and volume.
The Direct Patient Safety Risks of Inaccurate Documentation
The downstream consequences of medical documentation errors reach patients in ways that are often invisible until they cause harm. A wrong drug name becomes a contraindicated prescription at the next visit. A misrecorded allergy becomes an adverse reaction in the emergency department. A decimal error in pediatric dosing leads to hospitalization.
Medication-related adverse events cost between $38 billion and $50 billion in additional healthcare costs, disability, and lost productivity annually, according to StatPearls (2024). Medication errors were estimated to cause 1 in 131 deaths outside hospital settings and 1 in 854 deaths inside them. Transcription errors at the point of documentation are a consistent upstream contributor to those figures.
Documentation issues appear in 1 in 5 diagnosis-related malpractice cases, according to MedPro Group’s closed claims data spanning 2015 to 2024. The most common category is insufficient or missing documentation: gaps that leave clinical decisions undefended. A physician who saw the right finding but failed to document it is nearly as exposed legally as one who missed it entirely.
Why Healthcare Documentation Mistakes Compound Over Time
A single transcription error in an initial patient intake note can propagate through every subsequent visit. EHRs pull forward prior information, which means a wrong diagnosis code, an outdated medication list, or a missing problem item is automatically carried into the next encounter. The physician reviewing a returning patient sees what the chart says, not what actually happened six months ago.
Copy-paste behaviors and template overuse inside EHRs accelerate this pattern. Under documentation pressure, a physician copies yesterday’s note, updates a few fields, and unknowingly carries forward errors that were never caught. Clinical documentation accuracy is a systemic problem, not a one-time mistake.
Documentation and charting rank as the top burnout driver among physicians, according to Tebra’s 2025 Physician Burnout Survey. For every 15 minutes spent with a patient, physicians spend an average of nine minutes charting. That ratio does not produce careful, verified records. It produces fatigue, shortcuts, and downstream medical record errors.
The Financial and Legal Costs Hiding Inside Transcription Accuracy Failures
Healthcare documentation mistakes generate costs that practices rarely trace to their source. When a claim is rejected because the diagnosis code does not match the procedure code, the billing team reworks it. When a documentation gap triggers a malpractice case, the practice absorbs legal costs before the case is ever argued. These consequences rarely appear in any error report.
Verdicts over $10 million have more than doubled between 2015 and 2023, according to CM&F Group’s 2026 liability analysis, with the average award rising from $23 million to $40 million. MedPro Group confirms that documentation issues are a factor in 1 in 5 of those diagnosis-related cases.
Undercoding is a separate but related financial failure. When the transcription process misses supporting clinical detail from a complex visit, the resulting note cannot justify a higher-complexity billing code. Practices lose thousands per month through this mechanism, not through fraud, but through inaccurate clinical documentation that does not reflect what actually happened in the room. AI-assisted ICD-10 and CPT auto-coding exists precisely to surface the codes the visit supports before the chart closes.
Where AI Reduces Patient Safety Risks from Documentation Errors
AI medical scribes address transcription errors in healthcare at their source: the conversion of spoken clinical conversations into structured documentation. Ambient AI listens to the physician-patient consultation in real time and generates the clinical note, eliminating the manual transcription step and the errors it introduces.
Platforms like Notiro are built around this architecture. Notiro’s AI medical scribe captures the visit as it happens, generating SOAP, H&P, or POMR notes from the consultation audio rather than from post-visit dictation. The physician reviews an AI-generated note, confirms or corrects it, and syncs it to the EHR, with medication names, dosage figures, and clinical findings captured directly from the encounter.
A Mass General Brigham study found a 21.2% drop in physician burnout scores after 84 days of AI scribe use. Reducing documentation load produces more accurate records, not just faster ones. A physician who is not racing through nine minutes of charting per patient produces notes that are closer to what actually occurred.
Notiro extends beyond note generation. After each visit, it auto-suggests ICD-10 diagnosis codes and CPT procedure codes from the audio and note content, closing the loop between clinical documentation accuracy and billing. That is an area where most AI scribes stop entirely.
What Clinical Documentation Accuracy Requires in Practice
Consistent transcription accuracy in an outpatient setting requires the clinical note to be generated at the point of care, reviewed before chart closure, and connected to the billing workflow so documentation gaps are caught before they propagate.
AI scribe tools that only generate notes after the visit shift the transcription burden rather than remove it. A physician who dictates to an AI tool post-visit is still relying on recall, under the same cognitive load that leads to manual errors. Ambient scribing, where the AI listens during the visit, is a structural difference, not a feature comparison.
Notiro’s platform covers the full clinical day: patient intake before the visit, ambient scribing during the visit, and ICD-10/CPT coding after the visit. Healthcare teams using this workflow see fewer documentation gaps, faster chart closure, and less after-hours charting.
The Cost of Inaction on Medical Record Errors
Every practice relying on manual transcription is absorbing a baseline error rate it has probably never measured. The prescription and transcription stages are the most vulnerable points in medication management, according to hospital evaluation studies. Most errors are caught before they reach patients, but those that are not tend to cause the most serious harm and liability.
The question for any physician or practice manager is not whether transcription errors occur in their setting. They are. The question is: what percentage are caught before they affect a patient, trigger a claim, or generate a rejected billing code? That number is almost never tracked, so the actual cost stays hidden within the workflow rather than being visible on any dashboard.
Inaccurate documentation is one of the most consistent and measurable patient safety risks in outpatient medicine, and it compounds with every visit that builds on a flawed prior record. Notiro captures what actually happens in the room, generates the note, and closes the billing loop before the chart moves to the next encounter.
Start your free trial at Notiro.ai. No IT setup, no enterprise contract.