Psychiatrists spend an estimated 16 hours per week on documentation, among the highest of any medical specialty. That is not a rounding error. It is a structural problem, and it has a specific cause: psychiatric documentation does not look like a primary care note.
A 50-minute session with a patient managing treatment-resistant depression, a recent medication titration, and a disclosure of passive suicidal ideation produces several hundred words of clinically material content.
The Mental Status Examination (MSE) alone covers appearance, behavior, speech, mood, affect, thought process, thought content, perception, cognition, insight, and judgment, none of it reducible to a checkbox. The risk assessment requires a structured language precise enough to withstand legal and clinical scrutiny. The plan must be detailed enough to support the CPT code being billed.
General-purpose AI medical scribe tools for psychiatry were not designed for this. They were built on primary care workflows. The psychiatrist evaluating AI documentation for psychiatrists is not asking whether the tool can transcribe a session. They are asking whether it captures what actually happened in the room, and then codes it accurately enough to get paid.
What General AI Scribes Consistently Miss in Psychiatric Documentation
The ambient scribes built for high-volume primary care handle a specific pattern: chief complaint, history of present illness, physical exam, assessment, plan. That structure holds for a 15-minute acute visit. It does not hold for a 45-minute psychiatric evaluation.
- Mental Status Examination capture is the first point of failure. A general scribe may note that the patient “appeared anxious,” but miss the clinical distinction between constricted and flat affect, or between pressured and tangential speech. These are not interchangeable terms. They carry diagnostic weight and shape the clinical record. A psychiatric AI scribe must recognize the MSE domains in natural conversation and structure them correctly, rather than flagging them as miscellaneous narrative.
- Risk assessment documentation is the second. A note documenting passive suicidal ideation without capturing the safety plan, the SI/HI screening, or the clinical reasoning behind the discharge decision is incomplete and a liability. Most general scribes do not extract and structure risk language with the specificity required in psychiatric documentation.
- Note formats are the third gap. Psychiatry uses SOAP, as well as DAP (Data, Assessment, Plan) and BIRP (Behavior, Intervention, Response, Plan) formats, both built for therapy and behavioral health encounters. A scribe that only generates SOAP notes forces the clinician to reformat the output before it is usable.
- DSM-to-ICD-10 mapping is where all of this converges on billing. A note that reads “consistent with prior MDD presentation, single episode, moderate” needs to be resolved to F32.1 for billing purposes. That lookup, done manually at the end of a session day, under time pressure, is a systematic source of undercoding. According to CMS, ICD-10 contains over 70,000 codes, and CPT over 10,000, and psychiatric CPT codes for psychotherapy (90834, 90837) and medication management (99213, 99214) require documentation that explicitly supports the complexity level billed.
Notiro’s AI note-taking for psychiatrists addresses each of these gaps. The AI is trained on mental health clinical language, structures MSE and risk assessment content from session audio, and auto-suggests ICD-10 and CPT codes from the note before the chart closes.
The Burnout Reality Specific to Psychiatric Practice
The American Medical Association reports that 51% of US physicians experience burnout, and documentation is consistently named as the leading driver. In psychiatry, that burden compounds differently. The sessions are longer. The documentation is narrative and clinically dense. The cognitive carry from a session involving trauma disclosure or a safety assessment is real, and spending the following hour reconstructing it into a chart note amplifies it.
For many psychiatrists, the documentation burden begins the moment a session ends. What looks like a 50-minute appointment often triggers hours of additional clinical and administrative work.
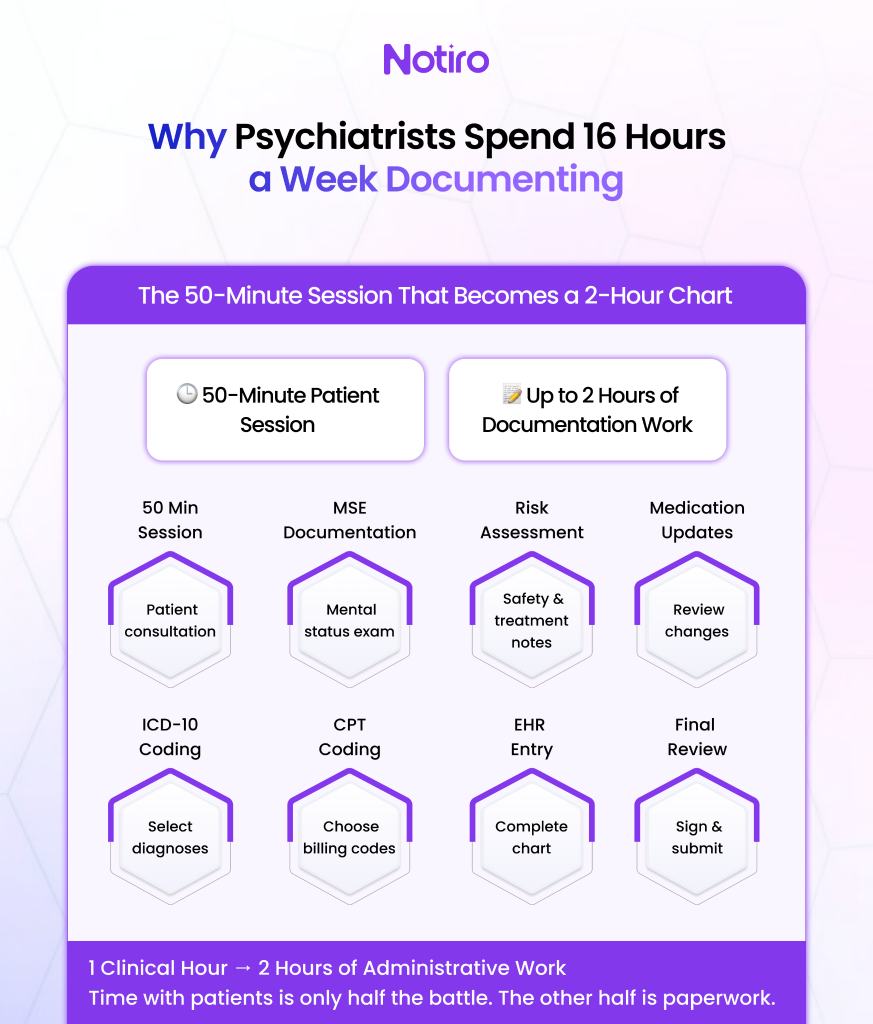
ALT TEXT: “ The 50-minute session that becomes a 2-hour Chart.”
A Mass General Brigham study found a 21.2% drop in burnout scores in physicians using AI scribes after 84 days. The same analysis found that 78% of clinicians reported less cognitive burden during visits. For the psychiatrist whose therapeutic presence is the treatment, that reduction matters beyond the time saved.
Physician burnout costs US healthcare $4.6 billion annually in turnover and productivity loss, according to an Annals of Internal Medicine analysis. A mental health AI scribe that reduces after-hours charting does not just return evenings, it changes the retention math for the practice.
The 50-Minute Session Shouldn’t Produce a 2-Hour Chart
Most AI scribe tools enter the workflow at the session level and exit at the note level. Notiro covers the clinical day from before the first patient to after the last chart closes.
Before the session, Notiro’s Patient Intake AI collects the patient’s presenting concerns, symptom history, and medication information directly. The psychiatrist walks in already briefed, not spending the first five minutes of a 50-minute session establishing what the patient is bringing that day.
During the session, the ambient scribe captures the conversation in real time. The note generates automatically in the appropriate format, SOAP, DAP, or BIRP, depending on the visit type, with MSE findings, risk language, and diagnostic impressions pulled from the audio. Telepsychiatry sessions are fully supported. Notiro works on mobile, with no hardware requirement, covering both in-office and remote visits without a workflow change.
After the session, ICD-10 and CPT codes surface automatically from the note content. The psychiatrist reviews, adjusts if needed, and the completed note and codes sync to the EHR in one click. Confirmed integrations include Athenahealth and Epic.
For medication management visits, one of the highest documentation-friction points in outpatient psychiatry, Notiro’s Prescription Intelligence captures titrations, refills, new prescriptions, and medication reconciliation directly from the session. These feed into the note and EHR sync without separate manual entry.
Where Notiro Stands on Coding, and Why That Matters More Than the Note
The honest competitive picture: ambient scribing is now available from dozens of tools. Freed AI, Heidi Health, and Nabla all generate clinical notes from session audio. None of them generates billing codes.
Automated ICD-10 and CPT coding from visit audio is Notiro’s primary differentiator. DeepScribe offers comparable coding automation, but at $350–$500 per provider per month, pricing built for health systems, not solo psychiatrists or small group practices. Notiro makes the same capability available at a practice size that actually describes most outpatient psychiatric providers in the US.
For the psychiatrist who spent 50 minutes with a patient and selected a level-3 code when the visit warranted level-4, not from negligence, but from time pressure and the sheer volume of manual code lookups, this is the gap that costs the most money. Notiro’s automated coding surfaces what the visit actually supports, before the chart closes.
HIPAA, 42 CFR Part 2, and Why Compliance Is More Than a Checkbox in Psychiatry
Psychiatric session audio contains some of the most sensitive Protected Health Information (PHI) in medicine. HIPAA requires that any vendor processing this audio sign a Business Associate Agreement (BAA). Without one, the psychiatrist is potentially in violation of federal law, regardless of what the scribe tool’s marketing materials say.
Notiro is HIPAA-compliant and provides a BAA with every practice’s onboarding. The HIPAA compliance page is public, and the BAA is available before any session data is processed.
Practices treating patients with co-occurring substance use disorders should also be aware of 42 CFR Part 2, federal regulations governing the confidentiality of substance use disorder records that impose stricter restrictions than standard HIPAA rules. Any psychiatry clinical documentation software operating in dual-diagnosis settings needs to address this layer of compliance. Confirm with the Notiro team for current 42 CFR Part 2 guidance specific to the practice’s patient population.
The Right Question to Ask Before Choosing a Psychiatric AI Scribe
The evaluation criteria that actually matter for psychiatric practice are these: Does the tool capture MSE content from natural conversation rather than just transcribe it? Does it structure risk language accurately enough to sign? Does it support DAP and BIRP in addition to SOAP? Does it generate billing codes, or stop at the note? And does it carry a BAA?
Most tools answer yes to one or two. Notiro answers yes to all of them.
Ready to Cut 16 Hours of Weekly Charting?
Psychiatric documentation carries more clinical, legal, and billing weight per word than almost any other specialty. The AI scribe that handles only the note is solving the easy part. Notiro covers MSE capture, risk documentation structure, automated ICD-10 and CPT coding, and medication management, from the first word of the session to EHR closure.
Start your free trial at notiro, no IT setup, no enterprise contract.