A rushed physician opens the last visit’s note and copies the assessment forward. It saves four minutes on a 12-patient day. It also starts the copy-paste EHR problem that follows the chart for years.
Up to 90 percent of clinicians say they routinely copy forward old documentation, according to physician surveys. Independent reviewers later trace some of those entries into diagnostic errors and malpractice claims. The habit is not about laziness at all.
It is a workaround for a system that never gave physicians enough time to write fresh notes. This article examines why EHR copy-and-paste issues keep recurring. It also explains what changes when an AI medical scribe writes the note instead.
The Scope of the Copy-Paste EHR Problem
Copy and paste is the most common documentation shortcut in modern EHRs. Surveys report routine use as high as 90% among practicing clinicians. A JAMA analysis of outpatient notes found over 80 percent of the text was copied from earlier entries.
That volume turns routine progress notes into long, repetitive documents. Reviewers call this note bloat, and it buries the details that actually matter for the current visit. Finding the real story inside a cloned chart takes real time.
A separate claims review tied close to a third of EHR-related malpractice cases to copy and paste. Average payouts in those cases ran near 450,000 dollars. That number reflects legal risk, not just messy charting.
Healthcare documentation challenges like this rarely manifest as a single, dramatic error. They appear as small inconsistencies that accumulate over dozens of visits. Eventually, one of those inconsistencies reaches a chart review or a malpractice claim.
How EHR Copy and Paste Issues Create Patient Record Inaccuracies
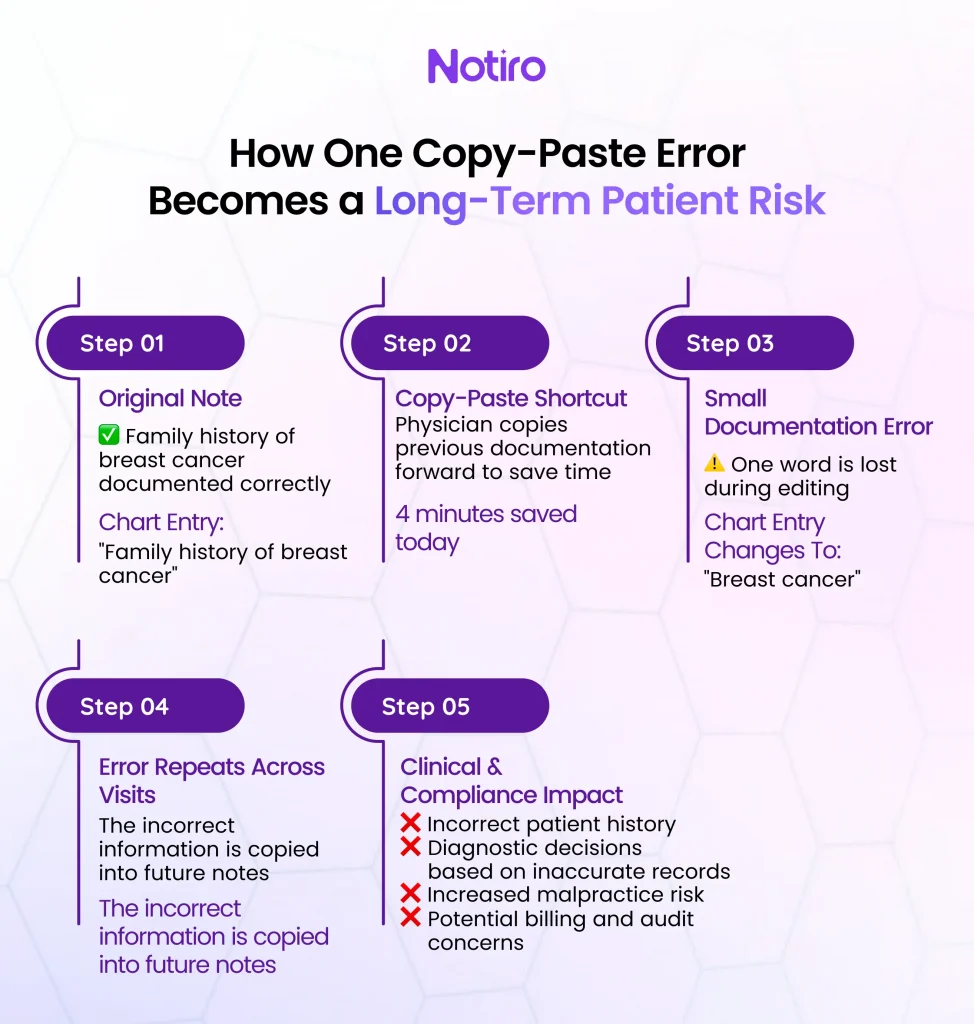
Picture a patient whose chart correctly notes a family history of breast cancer. A rushed copy and paste drops the word family, leaving just breast cancer in the active problem list. Every visit after that repeats the error, and no one catches it.
Researchers reviewing primary care charts linked copy-and-paste to a meaningful share of diagnostic errors. One frequently cited review attributed more than a third of flagged errors to copied or carried-forward text. Malpractice insurers now name copy and paste among the leading causes of EHR-related claims.
Carried forward documentation also creates billing exposure beyond the clinical risk. If a carried-forward note describes services that were not actually performed, the resulting claim can look fraudulent. Auditors do not distinguish between careless and intentional behavior.
Patient record inaccuracies like these do more than embarrass a single chart. They shape what the next physician believes about a patient before that physician walks in. Decisions about tests, referrals, and prescriptions follow from whatever the chart says was true.
Internal medicine and family practice charts carry the highest exposure to this risk. Multi-problem patients accumulate the most carried-forward text over time. A patient managing diabetes and hypertension may have vitals from last year sitting beside this morning’s symptoms.
Why Copy-Paste in Healthcare Documentation Has Become the Default
Copy-paste in healthcare documentation persists because the alternative costs too much time. Physicians already spend more than three hours a day on documentation and EHR work. Retyping a full history from scratch at every visit is not realistic at that pace.
EHR design itself encourages the shortcut even further. Templates and carry-forward fields are built into the chart specifically to save clicks. The tools meant to speed up documentation end up automating the very habit that damages it.
Vendors built carry-forward fields to help with older meaningful use requirements. Those same fields are now one of the most cited contributors to physician burnout. A habit introduced to save five minutes now costs entire evenings of chart cleanup.
An AI medical scribe changes that math by removing the retyping step entirely. Notiro listens to the actual visit and drafts a fresh, structured note in real time. The physician is no longer choosing between a fast note and an accurate one.
Clinical Documentation Accuracy and the Shift to AI-Generated Notes
Clinical documentation accuracy improves the moment the note stops being a copy of yesterday’s chart. Each Notiro note comes from that day’s conversation, including symptoms raised for the first time. Old negative findings and resolved problems do not carry forward by default.
The system supports SOAP, H&P, and POMR formats, so the structure matches how the physician already documents. It is built for clinical language, not general speech, which matters in a multi-problem visit. A diabetic patient with a new GI complaint receives a note that clearly reflects both issues.
Mass General Brigham measured a 21.2 percent drop in burnout scores after 84 days of scribe use. UCSF research found that scribe adopters earn about 3,000 dollars more per year and see one extra patient per week. Faster, more complete notes are part of why that gain shows up.
Fresh documentation also changes what happens after the note is written. A note that reflects today’s findings gives the next clinician a more reliable starting point for clinical reasoning. For complex, multi-problem visits, Notiro’s Diagnosis Support layer adds an extra checkpoint before the note is signed.
Closing the Loop: EHR Integration That Ends Electronic Health Record Errors
A finished note still has to land inside the chart without breaking the workflow. Many AI scribes stop at a copyable block of text that the physician has to paste manually. That manual step reopens the door to the same electronic health record errors this article started with.
Notiro syncs the completed note, along with suggested ICD-10 and CPT codes, into the EHR in one click. Confirmed integrations currently include Athenahealth and Epic, covering a large share of US outpatient practices. The chart is ready before the next patient sits down.
Manual post-visit coding is a known source of undercoding under time pressure. ICD-10 alone has more than 70,000 codes, and CPT adds 10,000 more, so guessing is common. Notiro suggests codes drawn from the actual visit, not a memorized shortcut list.
This works the same way across visit types, including in-person, telehealth, and walk-in encounters. A practice manager reviewing monthly billing sees codes tied to documented findings, not a default pattern. That traceability matters as much for an audit as it does for a single patient’s chart.
Cleaner, code-linked documentation also supports revenue integrity, not just compliance. Practices using AI-assisted coding tend to see fewer claim rejections and clearer audit trails. Notiro is also HIPAA compliant and signs a Business Associate Agreement with every adopting practice.
The copy-paste EHR problem will not disappear through better training alone. It changes when the fastest way to document also becomes the most accurate way. That is the bar an AI medical scribe should be measured against.
Every cloned note began as a shortcut on a day with no time to write a new one. Notiro removes that trade-off by generating a new note on each visit and syncing it to the EHR. Start a free trial at notiro and see what an accurate, same-day chart looks like.