Digital records were meant to simplify clinical work. As paper charts disappeared, EMR software promised faster access to patient information, better continuity, and more organized care delivery. In practice, however, many clinicians find that the documentation effort did not disappear. It shifted. What was once written on paper is now typed, reviewed, and corrected.
In order to understand what EMR software really does in clinical practice, one needs to separate record management from documentation creation. EMR systems are efficient in the organization and storage of medical information; however, these systems are dependent upon the clinicians to translate complex patient conversations into structured, compliant notes. This distinction demonstrates why documentation effort remains high even in digitally mature practices.
What is EMR software?
Electronic Medical Record (EMR) software is a digital version of paper charts used in the medical sector. The EMRs keep a thorough record of the conversation between doctor and patient, what was diagnosed, and how the treatment plan was formulated throughout the patient’s life cycle.
The EMR software holds the official record of the healthcare provided to any patients. This is significant as it ensures the continuity and the consistency required for proper medical procedure.
In addition to that, the practical framework of an EMR software system is not just the storage unit of information. It is where clinicians translate patient encounters into structured documentation, often after the visit, so that the record can be complete, compliant, and billable.
Despite the improved access, the EMR systems are dependent upon clinicians for manual entry of data and its interpretation.
Which Types of EMR Software Are Used in Healthcare
EMR platforms vary based on practice size, complexity, and operational needs. While functionality overlaps, deployment models and workflow depth differ.
- Practice-based EMR systems are designed for single clinics or small-group practices. The focus point of these EMR systems is on documentation of the patient history, scheduling follow-ups, and formulating bills.
- Enterprise EMR systems are used by hospitals and large health systems to support multidisciplinary workflows, specialty modules, and cross-site access.
- Specialty-specific EMRs are used in specified clinical domains, such as cardiology, mental health, or orthopedics.
- Cloud-based EMR systems are hosted remotely, enabling straightforward upgradesand cross-departmental access.
Benefits of EMR Software in Clinical Practice
EMR software delivers value once clinical information is entered and finalized. Its benefits are centered around record organization, compliance, and access.
- Centralized patient records
EMR systems help organize the whole medical history of a patient. This organization improves the continuity of care for patients. - Support for billing and reimbursement workflows
Structured records help ensure services are documented and align with coding and billing requirements. - Improved access to the patient’s medical history
Physicians can quickly review past visits, laboratory results, and treatments. This helps them rely less on memory and paper records. - Standardization across care teams
Using templates and structured fields helps keep documentation consistent among clinicians in the same organization.
EMR software organizes records, not conversations
Patient–doctor conversations rarely follow a structured form. Symptoms are often described in everyday language, with details emerging with the advent of time or in response to follow-up questions. EMR softwares are not built to capture these conversations as structured records. Instead, clinicians are required to interpret and encode these conversations into the system manually.
This means that in many workflows, clinicians still reconstruct encounters after the fact. The EMR becomes a “system of completion” rather than a system that reduces the work needed to produce high-quality documentation.
Why documentation effort remains high inside EMR platforms
Even with digital records, clinicians still:
- Navigate multiple screens and fields
- Type or dictate structured content
- Use templates that often need correction.
- Reconcile past and present information.
This effort becomes a recurring workload that many clinicians describe as documentation pressure rather than documentation support.
Research highlights:
Studies have shown that time consumed while interacting with electronic record systems often exceeds time spent in face-to-face patient care, and that this documentation burden is associated with clinician stress and burnout. Excessive documentation requirements and poor workflows are significant contributors to dissatisfaction and reduced well-being among clinicians.
How to Reduce the Documentation Burden of an EMR Software
Why documentation still feels manual
Despite digital tools, clinicians still type, click through fields, and correct notes to meet clinical, billing, and compliance expectations. Templates can catalyze the initial entry, but introduce boilerplate language later, which must be re-edited. In many practices, documentation remains a post-visit task, completed after patients have left.
This manual effort absorbs hours that clinicians would otherwise devote to patient engagement, clinical reasoning, and care planning.
Downstream impact of EMR documentation workflows
Documentation created inside EMR software systems affects more than clinicians. Medical notes that lack clarity and completion lead to:
- Coding queries
- Follow-up clarifications
- Administrative review
- Compliance reviews
These recurring tasks add work for clinicians and support staff. This doesn’t stop here; it leads to a ripple effect that increases overall operational load.
Why EMR software alone can’t resolve the documentation burden
EMR softwares organize as well as store medical records; however, they do to reduce the effort needed to create them. As long as documentation depends on manual entry, post-visit reconstruction, and template corrections, clinicians will continue to spend significant time on documentation, even outside normal clinical hours.
This is why many practices using the best EMR software systems struggle with after-hours charting and documentation fatigue.
How Clinicians Use EHR Software and Where the Gaps Appear
In day-to-day practice, clinicians use EHR software primarily as a reference point during patient encounters and as a documentation workspace after the visit. Before seeing a patient, they review prior notes, medications, and results to orient themselves. During the encounter, most interactions with the EHR are limited, as navigating screens or entering data can interrupt the conversation and clinical flow.
The bulk of documentation typically happens after the patient leaves. Clinicians translate the encounter into structured notes, reconcile templates, and ensure records meet clinical, billing, and compliance requirements. This post-visit reconstruction introduces pressure, especially in high-volume settings, and often pushes documentation into evenings or between appointments. While EHR systems organize and store information effectively, they do not reduce the effort required to create accurate notes. This gap is why many practices begin looking for tools that support documentation creation alongside the EHR, rather than expecting the EHR itself to solve the documentation burden.
How Tools That Support Documentation Can Complement EMR Software Systems
As we have established, EMR workflows are unable to reduce the documentation effort. Reducing documentation burden requires an AI transcription platform that works alongside existing EMR software.
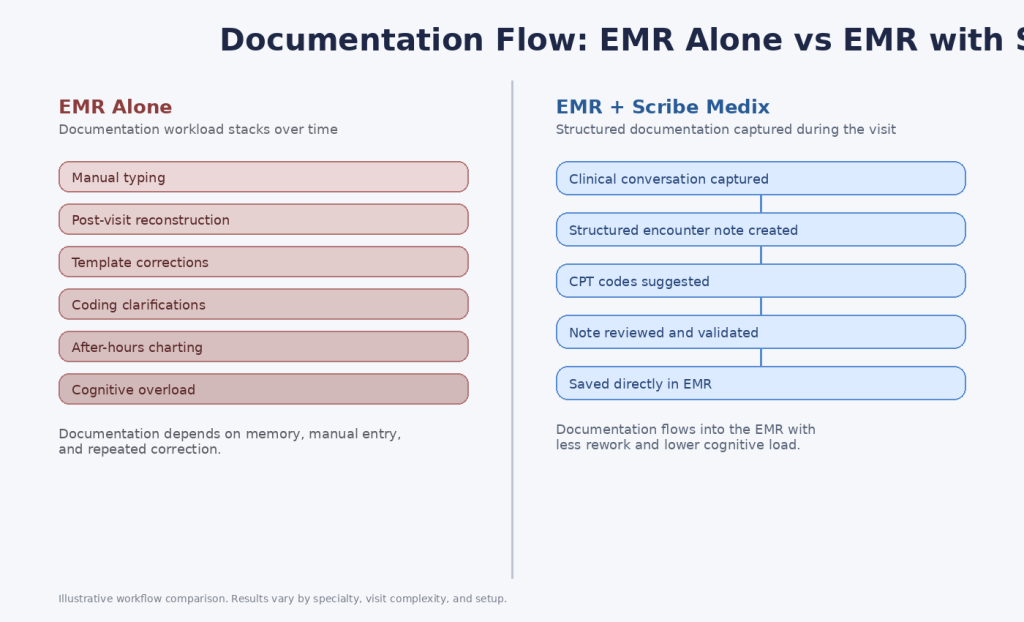
Solutions that capture clinical conversations and produce structured encounter notes and coding suggestions directly within the EMR can dramatically reduce manual typing and post-visit rewriting. Instead of reconstructing the visit from memory, clinicians can focus on doctor-patient interactions and accurate diagnosis.
“This approach allows practices to leverage their existing EMR infrastructure while reducing:
- After-hours documentation
- Post-visit rewriting
- Cognitive load associated with manual entry
- Downstream coding and compliance work”
Scribe Medix Supporting the EMR Workflows
Notiro is designed to complement EMR software platforms by supporting structured medical transcription from patient encounters while keeping clinicians free of unnecessary burden. By automatically creating encounter notes and suggesting CPT codes directly within the EMR, Scribe Medix eliminates much of the manual data entry traditionally required after the visit.
This means clinicians spend less time reconstructing conversations and more time interacting with patients and making clinical decisions. In busy practices and hospital environments where documentation effort remains high, Scribe Medix reduces the workload that EMR software alone does not address.





